Review written by Kimberly Sabsay (QCB, G3)
Socioeconomic status (SES), often simplified as absolute material wealth, is often linked to a variety of human health metrics. At a fundamental level, it makes sense that higher SES likely corresponds with access to better medical services, and in turn, better overall health. Studies have shown that, indeed, higher SES is associated with better human health, but the majority of this data comes from high-income countries (HICs). Despite the growing amount of scientific evidence for the apparent gradients in disease risk and survival explained by access to medical care and other health-related lifestyle factors, we cannot be certain that these trends are universal. Understanding the relationship between SES and health is crucial for policy design and to ensure we make economic decisions that do not negatively impact overall human health. Ultimately, the relationships between SES and health can be used to motivate positive change that benefits all of humanity.
It has been hypothesized that these wealth-based gradients in health observed in HICs are shaped by human evolution itself. Post industrial urbanization, the growth of globalized markets, and other modern advancements may directly amplify SES effects on health. For example, traditional small groups of hunters and gatherers tend to have strong kinship and synergistic lifestyles. This tends to be rarer in a modern society that limits upward mobility and, as a consequence of its densely populated urban environments, presents such challenges as racism, violence, and other social and political stressors. These factors may intensify stress in lower socioeconomic groups. Urbanization has also fostered a social stratification of healthcare resources largely absent during the pre-industrial era. Epidemiological changes that come with industrialization also affect the nature of SES-health relationships. It is more common, in modern society, to die from non-communicable diseases, rather than infectious disease, which remains the leading cause of death in pre-industrial societies. However, given the lack of studies done on the health effects of SES in lesser developed countries, the degree to which industrialization has altered SES-health relationships cannot be fully understood.
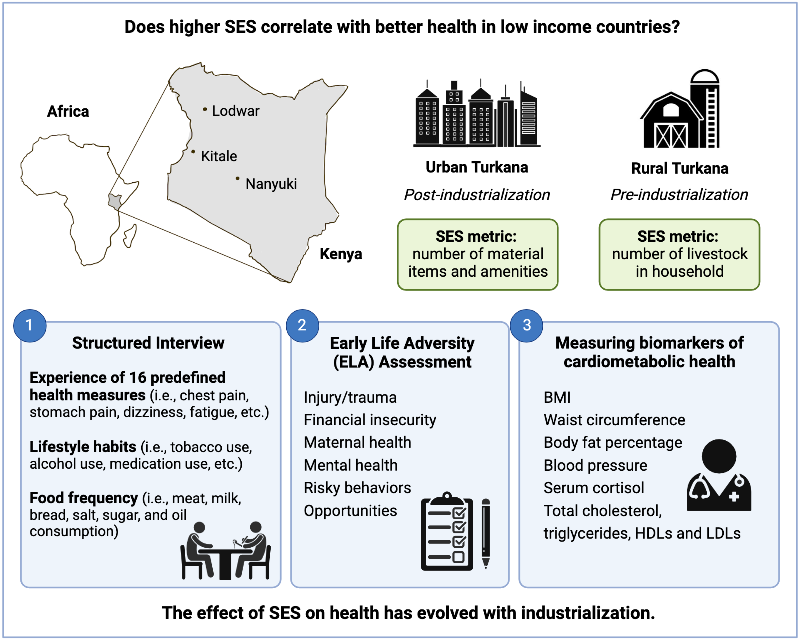
Researcher Amanda Lea and colleagues at Princeton University collaborated with researchers at the University of Nairobi and the University of California Santa Barbara to study the relationship between SES (defined as absolute material wealth) and health in Turkana: a small-scale, subsistence-level pastoralist population in northwest Kenya. Pastoralists are traditionally thought of as egalitarian and are portrayed as having equal and open access to natural resources, as well as a generous kinship across the community. However, intergenerational transmission of wealth inequality is just as present in Turkana as is observed in the most unequal HICs. In economics, the measure of wealth inequality within a social group is often measured by the Gini index, where a value of 0 represents perfect equality and a value of 1 represents maximal inequality. Pastoralists in Turkana have a Gini index of 0.42, whereas the US has an index of 0.37, demonstrating that despite the egalitarian appearance of Pastoralist groups, wealth disparity can still exist.
Thus, the goal of the study was to analyze the complex interplay between egalitarian social practices and high wealth variance to predict the relationship between SES and human health. Specifically, the researchers analyzed SES-health correlations in rural Turkana and examined how the correlations change when individuals transition to a more urban lifestyle. Recent economic and country-wide infrastructure expansions have caused many Turkana people to move to densely populated cities and adopt market-interfacing jobs over the past several decades, making the direct comparison between rural/Pastoralist and urban/industrialist Turkana possible. In this study, the researchers were able to test whether lifestyle change and human evolution influences SES-health relationships within a single population.
How the study was conducted
To provide more context, the Turkana have resided in northwest Kenya since the early 18th century. In general, Turkana county is semiarid with low annual rainfall and high year-round temperatures. The Turkana people are nomadic pastoralists, relying on dromedary camels, zebu cattle, fat tailed sheep, goats and donkeys for subsistence. As a result of this lifestyle, the Turkana diet is high in protein with about 70-80% of their calories coming from animal products.
The recent urbanization of surrounding areas have pulled Turkana people into the market-integrated cities. The study defines “urban” individuals as those who reside in the cities of Nanyuki, Lodwar, or Kitale and who no longer practice pastoralism. Non-pastoralists who reside in suburbs in Laikipia county were also classified as urban due to the cosmopolitan nature of this area. The study defines “rural” individuals (or “pastoralists”) as residents of Turkana county who self-report their main subsistence activity as pastoralism; essentially those who own livestock and rely on said livestock for food. It should be noted that the people who choose to move to urban areas represent a nonrandom subsample of the Turkana population and consequently, unaccounted for economic and social considerations that motivate individuals to migrate could result in population bias.
Data collection for the study occurred between April 2018 and February 2020, during which time researchers visited locations where Turkana individuals were known to reside. With discussion and approval from the local chiefs and elders of each community, all adults (>18 years old) with self-reported Tukana ancestry were invited to participate in the study. A total of 787 individuals participated in the study with 325 individuals classified as “pastoralist” and 462 individuals as “urban”. The study involved a structured interview, blood sample collection, and anthropometric measurements.
All structured interviews were conducted in a language familiar to the participant and relevant variables collected included: sex, age, main subsistence activity, highest education level, number of surviving children, number of wives (men only), use of contraceptives (women only), use of medications or medical treatment in the last month, alcohol and tobacco consumption, as well as experience of 16 specific health concerns within the last 3 months. In addition, a food frequency questionnaire collected information on the individual’s diet, specifically the consumption of meat, milk, bread, sugar, salt and cooking oil. Individuals were interviewed about their early life experiences using an adaptation of the Center for Disease Control’s Adverse Childhood Experiences (ACEs) assessment tool. For each individual, the number of predefined adverse childhood (<12 years old) experiences were tallied to quantify ELA.
Defining absolute material wealth is a complex and challenging process. Due to the nature of the two population groups within this study, the same metric for SES could not feasibly be used, which inherently limits the ability to directly compare the final results of the study. For pastoralists, wealth is concentrated in livestock holdings while urban dwellers generally possess their wealth in material items. Essentially, no urban Turkana individual would be considered wealthy if measured by the number of livestock holdings, and likewise, no rural Turkana individual would be considered wealthy if measured by the number of material possessions. Thus, the approach to define SES for this study relies on separate metrics for each social context. Among pastoralists, livestock are the primary source of material wealth, thus pastoralist SES was defined as the number of multispecies livestock owned by the household that the individual belonged to. To account for skew, due to the uneven distribution of wealth previously illustrated by the Gini index, the values were log2 transformed. This measure of SES was strongly correlated with other possible metrics of material wealth like estimated market prices and the ratio of livestock holdings to the number of household members, illustrating the strength of this measurement as a predictor of rural material wealth. Among market-integrated individuals in urban settings, a tally of material goods, dwelling characteristics and other household assets (e.g., electricity, TV, indoor tap water, etc.) was used as an index for SES and absolute material wealth. The specific list of material items and dwelling characteristics utilized has been widely used in previous studies, and results in a single value ranging from 0 (low SES) to 11 (high SES). This urban SES definition is strongly associated with education levels, which is another common measure of SES in industrialized settings, again illustrating the strength of this measurement as a predictor of urban material wealth.
Study results
The study’s results were somewhat unexpected. Within rural Turkana, SES is positively associated with self-reported health metrics. However, there are no significant relationships between SES and measures of cardiometabolic health (although most were generally healthy). By comparison, there are no significant associations between SES and self-reported health in urban Turkana (although the frequency of self-reported health issues is higher than in the rural subpopulation). Surprisingly, within urban Turkana, high SES is associated with low cardiometabolic health biomarkers. This is contrary to what studies in HICs have shown, where high SES is associated with greater cardiometabolic health. Additionally, the study deemed there is no significant association between SES and serum cortisol (a metric of happiness) in either rural or urban Turkana settings.
In terms of reproductive success metrics, higher SES in rural Turkana has no significant impact on the number of offspring, whereas higher SES in urban Turkana is associated with fewer offspring. These trends are likely explained, at least partially, by industrialization and SES effects on contraceptive usage and the frequency of polygyny.
To further understand the context dependent relationships seen within the collected data, the researchers looked for potential mediators, or specific variables that may explain the trends and correlations. In statistics, a correlation is defined as a direct relationship between an independent variable and a dependent variable. Mediation analyses seek to explain data by introducing a mediator variable between the independent variable and dependent variable. In this model, the mediator variable is influenced by the independent variable and in turn influences the dependent variable. The independent variable of interest within this study is the quantified SES and dependent variables would include all of the measures of cardiometabolic health and reproductive fitness. Potential mediator variables of interest are serum cortisol levels and other sociobehavioral variables like tobacco use, diet, ELA, and available resources.
Several potential mediator variables were found to have significant or marginal associations with SES and were selected for formal mediation analysis. These variables included: (1) greater usage of salt, sugar and oil among low SES pastoralists and (2) greater consumption of meat, bread, and milk in addition to greater reliance on salt, sugar and oil among high SES individuals in urban Turkana. Minimal evidence for mediation was found with the exception of salt, sugar, and oil consumption explaining about 11% of the effect of SES on waist circumference in urban Turkana. In other words, the larger waist circumference of those of higher SES in urban Turkana is partially due to the increased consumption of salt, sugar, and fat.
A large number of studies have pointed to an association between adverse childhood experiences and early death in HICs. However, this novel study shows that there is generally no relationship between ELA and overall health in either Turkana setting. In terms of early life adversity, individuals within rural Turkana experienced greater cumulative ELA relative to those living in urban Turkana. 11.1% of pastoralist women and 15.6% of pastoralist men experienced five or more adversities while only 6.3% of urban women and 2.9% of urban men experienced the same level of hardship in early childhood. Age of participants within the study also correlated to an increase in cumulative ELA, suggesting the prevalence of childhood adversity has decreased over time. These results show that overall, cumulative ELA is patterned by lifestyle, however, there are no significant findings that ELA impacts adult health within the population sample as is seen in HICs.
Overall, the researchers examined SES-health associations within a population undergoing rapid lifestyle change to determine if industrialization has impacted the way SES is correlated to human health. Previous research, within HICs, has predicted that low SES is associated with worse health in both urban and rural settings, with these results exacerbated in the urban setting. The study found strong evidence that the recent transition from pastoralism to an industrial lifestyle does alter the relationship between absolute material wealth and health among the Turkana. Within rural Turkana, no significant relationship between SES and cardiometabolic health was found, whereas, individuals in urban Turkana with high SES actually had worse cardiometabolic health, displaying a trend opposite to predictions. The study therefore determines that the presence and direction of SES effects change as a function of lifestyle.
The researchers speculate that in pastoralist communities, wealth is likely directed into traditional food, family growth and resources that positively influence self-reported health, as well as that higher SES in this setting may allow for individuals to better cope with ecological hardship. Within the urban setting, it is speculated that wealth is directed into consumption and amenities that negatively impact cardiometabolic health (like processed foods and less physical exertion).Unfortunately, this is also consistent with studies that show that newly developed countries suffer an increased burden of non-communicable disease due to epidemiological and nutritional transitions.
The lack of significant findings from serum cortisol measurements remains an area of high interest and future work. The researchers speculate that increased sample sizes may help capture context-dependency of cortisol levels across lifestyle groups. Additionally, the apparent absence of significant sociobehavioral mediators of the SES-health relationship opens the door for the future analysis of many other possible mediation variables, like level of support and kinship, which likely varies with lifestyle but was not captured in this study. Overall, the study shows that the relationships between SES and human health in low-income countries differs from those in high-income countries and that these effects have evolved with industrialization.
Notes from a discussion with Dr. Amanda Lea:
When asked how her research has “evolved” (pun intended) now that she is at Vanderbilt University, lead author Amanda Lea said: “I am still very interested in how experiences over the life course (social, ecological, nutritional, etc) influence long-term health outcomes, and how lifestyle change is altering these relationships in subsistence-level groups. As a faculty member, I am now working with other large, international, collaborative projects to study these same questions in other groups (specifically the Tsimane of Bolivia and the Orang Asli of Malaysia). I am excited about developing these parallel projects to understand both generalities and differences across cultures and ecological contexts.”
Amanda also gave special thanks to the Mpala Research Centre in Laikipia, Kenya, without which the project would not have been possible.
Figure was created with BioRender.
The original article discussed here was published in Evolution, Medicine, and Public Health on November 25, 2021 . Please follow this link to view the full version.